Acute eosinophilic pneumonia (AEP) is a rapidly progressive inflammatory lung condition characterized by an abnormal accumulation of eosinophils—a type of white blood cell—in the lung tissue and air spaces. This disorder has been increasingly linked to vaping, particularly after initiation or intensification of e-cigarette use.
Mechanism & Causes
AEP after vaping occurs due to an immune-mediated hypersensitivity reaction to inhaled substances. Key pathophysiological processes include:
- Inhalation of irritants: E-cigarette aerosols contain ultrafine particles, flavoring chemicals (e.g., diacetyl), heavy metals (e.g., nickel), and solvents that directly injure lung epithelium.
- Eosinophil recruitment: Damaged tissues release cytokines (IL-5, IL-33, GM-CSF), triggering bone marrow production and pulmonary infiltration of eosinophils.
- Inflammatory cascade: Activated eosinophils release cytotoxic granules causing alveolar damage, capillary leakage, and non-cardiogenic pulmonary edema.
Risk factors include new vape device use, recent flavor changes, high-frequency vaping, and pre-existing respiratory conditions.
Symptoms
Symptoms develop within hours to weeks of vaping exposure and mimic severe pneumonia:
- Acute respiratory distress with hypoxia requiring supplemental oxygen
- Dry cough and pleuritic chest pain
- Fever (>38°C) and systemic malaise
- Tachypnea (>20 breaths/min) and tachycardia
Diagnosis
Diagnostic criteria combine clinical, radiographic, and laboratory findings:
- Bronchoalveolar lavage (BAL): Gold standard showing >25% eosinophils in BAL fluid.
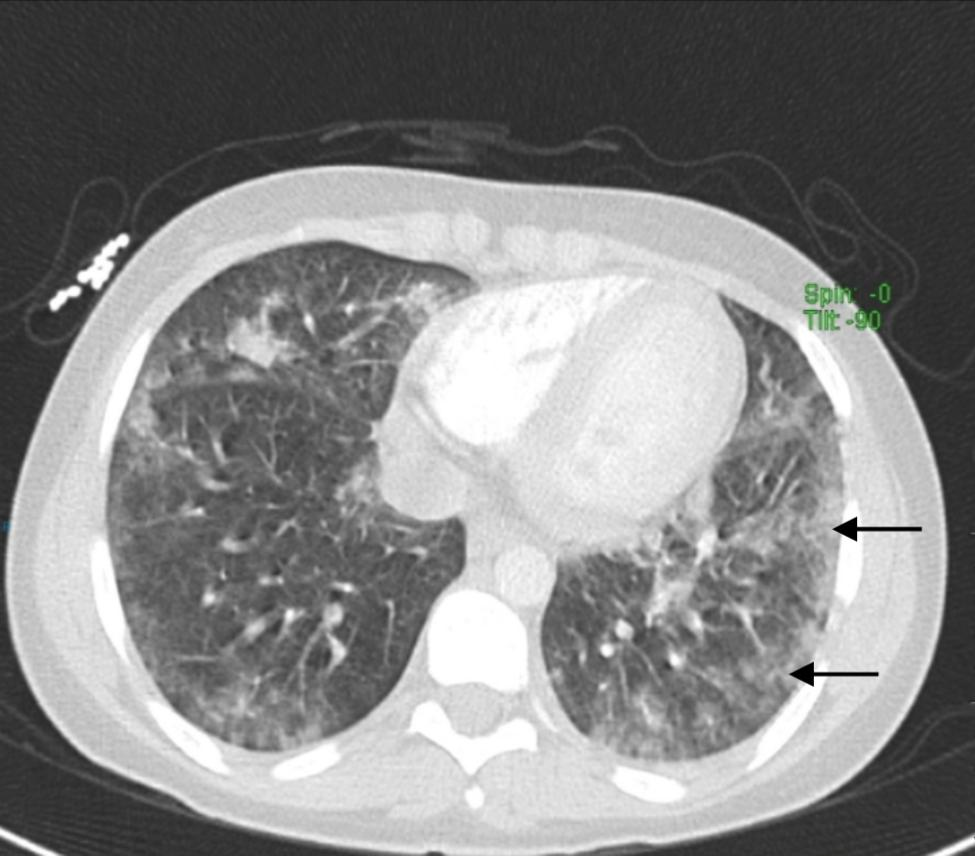
- Chest imaging: CT reveals diffuse ground-glass opacities and interlobular septal thickening.
- Blood tests: Peripheral eosinophilia occurs in most cases within 48 hours.
Vaping history and exclusion of infections (fungal/parasitic) are critical to confirm diagnosis.
Treatment
Immediate vaping cessation is mandatory. Medical management includes:
- Corticosteroids: Intravenous methylprednisolone (60-125mg every 6 hours) for severe cases, transitioning to oral prednisone (0.5-1mg/kg/day) with 1-3 month taper.
- Supportive care: Oxygen supplementation and mechanical ventilation if respiratory failure occurs.
Most patients show dramatic improvement within 48 hours of steroid initiation, though relapse occurs with resumed vaping.
Prevention
Complete abstinence from vaping is the only definitive preventive measure. Clinicians should educate patients about vaping-associated lung injury risks, particularly new users. Regulatory measures targeting flavorings and aerosolized chemicals may mitigate population-level risks.





